University of Pittsburgh
Human Engineering Research Laboratories
7180 Highland Drive 151R1-H Pittsburgh Pennsylvania 15206
United States
ABSTRACT
Wheelchair transfers have been associated with the high incidence of upper limb pain among persons with spinal cord injury. This study investigated hand and feet kinetics for three types of lateral transfers (two of which incorporated the head-hips relation and the third being translational), while comparing it to preferred method of transferring. Four persons with paraplegia performed each transfer while force sensors recorded the forces applied by the hands and feet. Peak and average resultant and vertical forces at the feet and hand were not significantly different across the transfer techniques. A pattern of feet forces being consistently higher for the HH-A technique compared to the SS and taught transfer techniques was found to exist. Greater off loading through the lower extremities using this transfer technique could potentially preserve upper extremity function. Future studies that include larger sample size and 3D kinematics of the trunk are required to confirm findings.
KEYWORDS
Biomechanics, feet, spinal cord injury, activities of daily living.
BACKGROUND
People with lower limb dysfunction, like spinal cord injury (SCI), commonly have upper limb pain, due to high reliance on their arms to perform activities of daily living such as wheelchair propulsion, pressure relief and transfers [1]. Being able to transfer independently is a key factor in achieving an optimal level of independence. Therefore upper limb pain can severely affect overall functional mobility and independence.
There are different approaches that are used to perform transfer activities such as the lateral, front or back. The lateral transfer is the most common as it is quick and requires less strength. Lateral transfers are considered essential for maintaining an independent lifestyle [2]. Allison et al. [3] described two general movement strategies used when performing lateral transfers: rotational strategy (head moves in an opposite direction to the pelvis) and translational strategy (head and pelvis move simultaneously in the same direction). When viewed from the sagittal plane, individuals performing the rotational strategy leaned forward during the transfer and those using the translational strategy kept their trunk more upright during the transfer. The rotational strategy is analogous to what clinical practice refers to as the ‘head-hips’ relation. It is often taught to patients with weak triceps and/or those with high levels of trunk involvement. Using a forward-flexed trunk position during transfers and pressure relief engages sternal pectoralis major and latissimus dorsi muscles [3]. This muscle substitution may help transfer the body weight between the leading arm (arm reaching to new surface) and trailing arm (arm behind during move to new location) with less loading of the glenohumeral joint thereby reducing the risk of rotator cuff impingement [3, 4].
Clinical Practice Guidelines discuss the importance of accommodating a fixed position of lower extremities (LE’s) for improved balance and stabilization while performing activities of daily living [5]. Limited literature is available exploring the function of LE’s while performing wheelchair transfers. The purpose of this study was to investigate the role of LE’s while performing different lateral level transfer techniques:
- To compare hand and feet kinetics for three lateral level wheelchair transfer techniques:
- the head-hips relation where the leading arm is abducted and away from the body (HH-A) and again with the leading arm close to the body and internally rotated (HH-I) and the third technique was translational in nature where the trunk remained upright and leading arm abducted and away from the body (TU)
- To compare hand and feet kinetics for each taught transfer to the participant’s own method of lateral transfer.
We hypothesized that there will be greater off loading through the feet while performing the head hips transfer techniques compared to the trunk upright transfer technique.
METHODS
Subjects:
After reading and providing written informed consent, four subjects with SCI (3 male & 1 female), participated in this study. The inclusion criteria were: spinal cord injury C4 level or below that occurred over one year prior to the start of the study, able to independently transfer to/from a manual wheelchair without human assistance or assistive devices, over 18 years of age, and free from upper extremity (UE) pain that influenced their ability to transfer.
Experimental Protocol:
Participants used their personal wheelchairs to transfer to and from a bench. For all transfers the wheelchair was positioned and secured at a comfortable angle to an adjustable height tub bench as shown in Figure 1. The bench was adjusted to be level with the subject’s wheelchair seat. The kinetic measurement system consisted of three force plates (Bertec Corporation, Columbus, OH), one beneath the wheelchair, one beneath the tub bench and thirdly one located below the feet. The wheelchair and bench were secured to aluminum platforms which were bolted to the force plates. A steel beam attached to a 6-component load cell (Model MC5 from AMTI, Watertown, MA) was positioned to simulate a wheelchair armrest.
All transfers began with the left arm leading and moving the body from the wheelchair to the bench. For the first transfer, subjects were instructed to perform a lateral transfer as they normally would from their wheelchair to the adjacent level tub bench. For this transfer, they could place their left hand anywhere on the bench and right hand on the steel beam (height of wheelchair arm rest). The other three transfers were performed in random order. Prior to performing each of the transfer techniques, subjects were shown an instructional video on how to complete the transfer. For the Head Hips-A (HH-A) transfer, subjects were instructed to place their left hand on the far target of the bench, right hand on the target on the force beam, and transfer leaning their trunk forward as far as possible while moving their buttocks toward the large target on the bench while moving their head in the opposite direction (figure 1a). The Head Hips-I (HH-I) transfer required the same instructions except that the left hand was placed on the near target of the bench, with the left arm internally rotated (figure 1b). For the Trunk Upright (TU) transfer subjects were instructed to place their left hand on the far target of the bench, right hand on the target on the force beam, and transfer with their trunk upright while moving their buttocks toward the large target on the bench; moving their head in the same direction (figure 1c). Each transfer technique was performed five times and kinetic data were recorded at 360 Hz, for the length of the transfer.
Data Analysis:
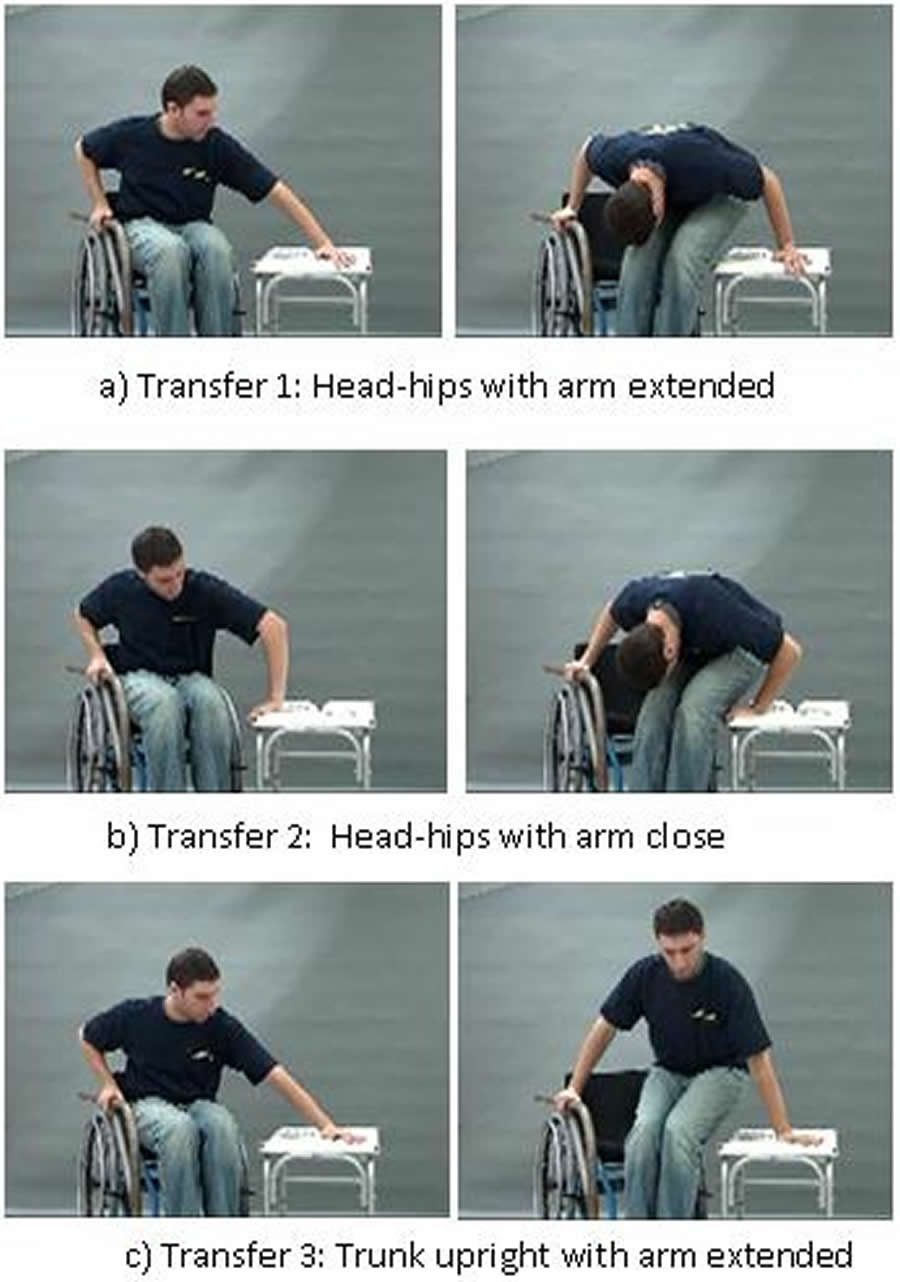 Figure
1. Still photos from the transfer instruction video for the three taught
transfer techniques.
Figure
1. Still photos from the transfer instruction video for the three taught
transfer techniques.Kinetic data were filtered with a 4th order zero-lag Butterworth filter with a cut off frequency of 5 Hz. The beginning and the end of each transfer was determined from the vertical force data from the force plate under the tub bench and the force-sensing beam. The increase of the forces followed by the decrease determines the lift phase of the transfer, where the arms are weight bearing [6]. The analysis was limited to data from the wheelchair to tub bench transfer averaged across the five trials. Peak and average forces for the hand components and resultant force for both leading and trailing hands as well as the feet were calculated for each transfer to the tub bench. In addition a hand to feet force ratio was calculated. Variables were computed using Matlab (Mathworks, Inc., Natwick, MA).
Statistical Analysis: Group means and standard deviations were determined for clinical and demographic characteristics. Differences between the four types of transfers among the kinetic variables for the hands and feet were evaluated using a repeated measure Friedman Test. A significance of less than 0.05 was selected. The statistical tests were performed using SPSS statistical software (SPSS Inc., Chicago, IL).
RESULTS
Subjects
A group of 4 manual wheelchair users with a mean (± standard deviation) age, weight and height of 45.00 (± 11.55) years, 71.35(± 11.43) kilograms and 1.74 (± 0.09) meters participated in this study. The sample had lesion levels varying between T7 – L5.
Differences in transfer techniques
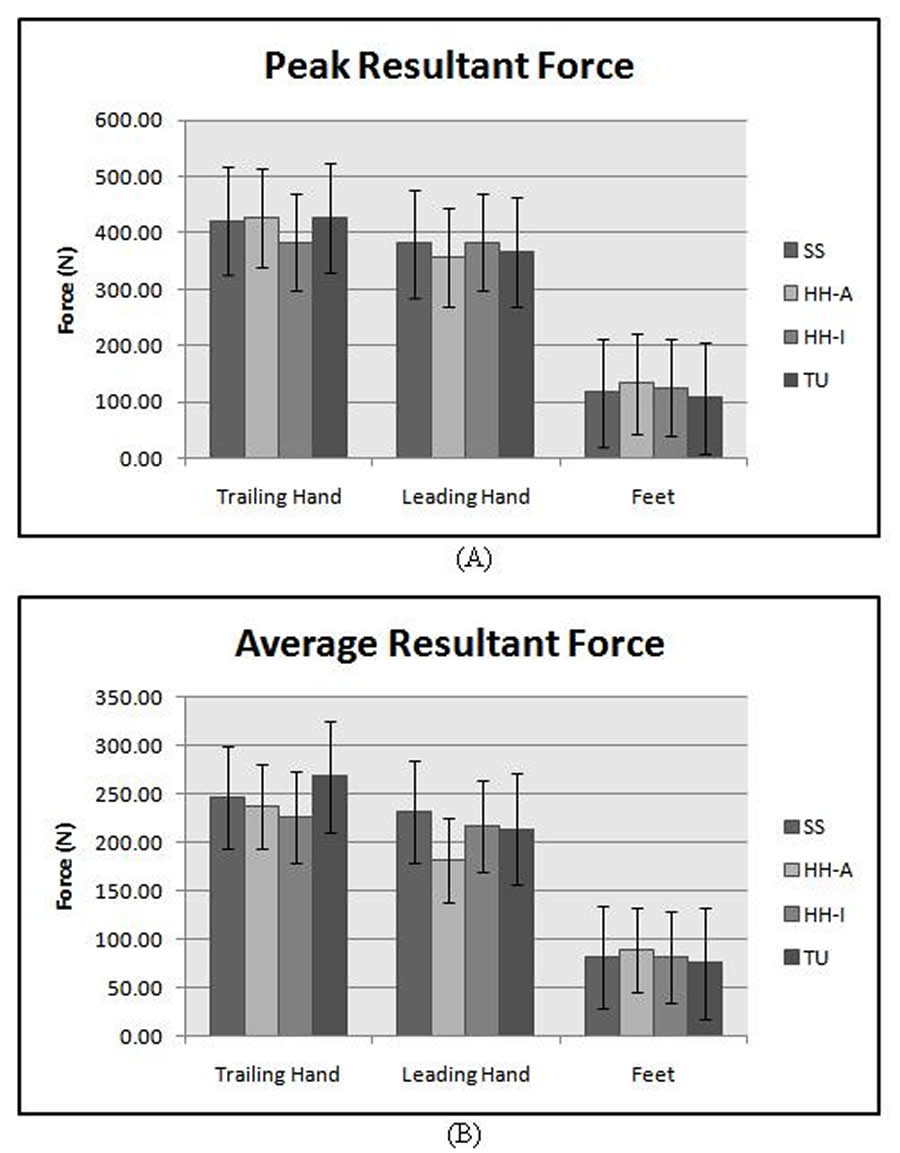 Figure 2. Maximum and average resultant force borne at the hands and
feet showed no significant differences across transfer techniques.
A trend of higher forces exhibited during the HH-A transfer at feet
were observed.
Figure 2. Maximum and average resultant force borne at the hands and
feet showed no significant differences across transfer techniques.
A trend of higher forces exhibited during the HH-A transfer at feet
were observed.Analysis was limited to the vertical reaction forces owing to the fact that this component was considerably higher at the hands and feet compared to the antero-posterior and medio-lateral force components. Resultant forces borne at the hands and feet for each transfer technique are shown in figure 2. The peak and average resultant and vertical forces at the feet and hand were not significantly different across the transfer techniques. We did find a trend that the feet forces were higher for the HH-A technique compared to the SS and taught transfer techniques.
The hand to feet ratio for the vertical and resultant force components for each transfer technique is listed in Table 1. The ratios showed that by and large the reaction forces borne at the hand were three times the magnitude experienced at the feet.
The HH-A technique resulted in the lowest hand to feet ratios compared to the remaining techniques indicating that the feet had greater off loading compared to the UE’s. The maximum and average vertical reaction forces, in terms of % body weight (%BW), supported by the feet were greatest for the HH-A technique (18.44% & 12.51%) compared to the HH-I (17.23% & 11.41%), SS (16.23% & 11.78%) and the least being TU (14.7 % & 10.79 %). Similarly the maximum and average resultants forces at the feet were highest for the HH-A technique (19.06 % & 12.82%) compared to the HH-I (17.82 % & 11.66%), SS (15.73% & 11.18%) and TU (14.7 % & 10.79 %).
DISCUSSION
The purpose of this study was to investigate lower extremity loading for Head Hips-A&I and TU transfers and to compare the self selected transferring techniques to the taught transfers. Although no significant differences were found between forces borne at the feet across transfer techniques it was interesting to note that the forces were consistently higher for the HH-A technique compared to the remaining transfer techniques. As hypothesized, we found more LE weight bearing during the head hips transfer techniques compared to the TU technique.
Gagnon et al [7] explored the role of the feet during level and non-level transfers and found that average and peak vertical forces were significantly higher at the hands compared to the feet. Similarly for the level transfers investigated in this study, majority of the weight bearing during the lift phase of the transfer occurs at the hand compared to the feet across all the transfer techniques. This study not only analyzed participants preferred method of transferring but also taught techniques. We found that the LE’s bear close to 17 % BW while transferring with the SS technique as compared to the approximate estimation of 30% BW as stated by Gagnon et al.
Variables |
Hand: Feet |
SS |
HH-A |
HH-I |
TU |
|---|---|---|---|---|---|
Peak Resultant Force |
Trail Hand: Feet |
3.60 |
3.20 |
3.07 |
3.95 |
Lead Hand: Feet |
3.26 |
2.67 |
3.07 |
3.40 |
|
UE: Feet |
3.43 |
2.94 |
3.07 |
3.68 |
|
Average Resultant Force |
Trail Hand: Feet |
3.03 |
2.69 |
2.80 |
3.56 |
Lead Hand: Feet |
2.86 |
2.04 |
2.68 |
2.84 |
|
UE: Feet |
2.95 |
2.37 |
2.74 |
3.20 |
|
Peak Vertical |
Trail Hand: Feet |
2.70 |
2.58 |
2.64 |
2.70 |
Lead Hand: Feet |
2.42 |
1.91 |
2.16 |
2.42 |
|
UE: Feet |
2.58 |
2.52 |
2.55 |
2.58 |
|
Average Vertical Force |
Trail Hand: Feet |
2.70 |
2.42 |
2.58 |
3.34 |
Lead Hand: Feet |
2.58 |
1.91 |
2.52 |
2.79 |
|
UE: Feet |
2.64 |
2.16 |
2.55 |
3.06 |
|
| *UE- Forces averaged across trailing and leading hands | |||||
In previous studies exploring UE kinetics during lateral level wheelchair transfer techniques, led us to believe that the cohort of manual wheelchair (MWC) users adopted a more translatory manner as their selected method of transferring [8]. This can be corroborated by the findings of this study where the ratio variables computed for the SS technique actually fall within the TU and HH-I transfer techniques, which leads us to believe that preferred method of transferring varied between the aforementioned taught techniques. An additional finding from earlier studies where the two head hips method of transferring were compared to the TU technique found that transferring with the HH-A technique results in reduced hand and shoulder forces [9]. Therefore summarizing the previous and current study findings, we see that by transferring with HH-A technique results in reduced UE forces and greater off loading through the LE’s, which would potentially lead to preservation of UE function.
The results of this study highlights the importance of the LE’s during transfers as they are being used to support close to 20 % BW (averaged across the techniques), during the transfer.
Although the sample consisted of an experienced group of manual wheelchair users, owing to the small statistical power, it is difficult to draw conclusive results. Future studies involving more subjects and additional variables such as trunk kinematics and shoulder kinetics will assist in the analysis. The influence of balance and UE strength will also be taken into consideration to have a better understanding of the role of LE’s with respect to wheelchair transfer techniques
REFERENCES
- Davidoff G, et al. (1991). Compressive mononeuropathies of the upper extremity in chronic paraplegia. Paraplegia, 29, 17 24.
- Somers MF, Spinal cord injury functional rehabilitation, 2nd Ed., Prentice-Hall, Inc., Upper Saddle River, NJ 2001.
- Allison, GT and Singer KP, Assisted reach and transfers in individuals with tetraplegia: towards a solution. Spinal Cord 35, 217-222 (1997).
- Gagnon, D., Nadeau, S. , Gravel, D. , Noreau, L., Lariviere, C. Biomechanical analysis of a posterior transfer maneuver on a level surface in individuals with high and low-level spinal cord injuries. Clin Biomech 18, 319-331 (2003).
- Preserving Upper Limb Function in Spinal Cord Injury: A Clinical Practice Guideline for Health-Care Professionals, in Spinal Cord Medicine, Clinical Practice Guideline. 2005, Consortium for Spinal Cord Medicine
- Koontz, A.M., Kankipati, P., Cooper, R.A.,Custom measurement system for investigating wheelchair transfer biomechanics; Proceedings of ICMMB 2008 Annual Conference, Pittsburgh, PA, (July 23-25, 2008).
- Gagnon, D., Nadeau, S., Noreau, Dehail, P., Gravel, D. Quantification of reaction forces during sitting pivot transfers performed by individuals with spinal cord injury. J.Rehabil Med, 40, 468-476 (2008).
- Kankipati, P., Koontz, A.M., Boninger, M.L., Lin, Y.L. Hand and shoulder joint kinetic analysis of three types of lateral wheelchair transfers; Proceedings of RESNA 2009 Annual Conference, New Orleans, Louisiana, June 23-27, 2009.
- Kankipati, P., Koontz, A.M., Turkovich, M., Shoulder joint loading for three types of lateral wheelchair transfers; Proceedings of RESNA 2008 Annual Conference, Arlington, VA (Washington, DC ), June 26-30, 2008.
ACKNOWLEDGEMENTS
Funding for this study was provided by the Department of Veteran Affairs
(A4489R). This material is the result of work supported with resources
and the use of facilities at the Human Engineering Research
Laboratories, VA Pittsburgh Healthcare System.
Padmaja Kankipati, MS
Graduate Research Engineer
Human Engineering Research Laboratories
VA Pittsburgh Healthcare System & University of Pittsburgh
7180 Highland Drive, 151R1-H
Pittsburgh, PA 15206
Phone: (412)-954-5311
Fax: (412)-954-5340